Regional
The RSV shot shortage isn’t just a supply problem
The broken US health care system is a long-term barrier to Beyfortus vaccine access.
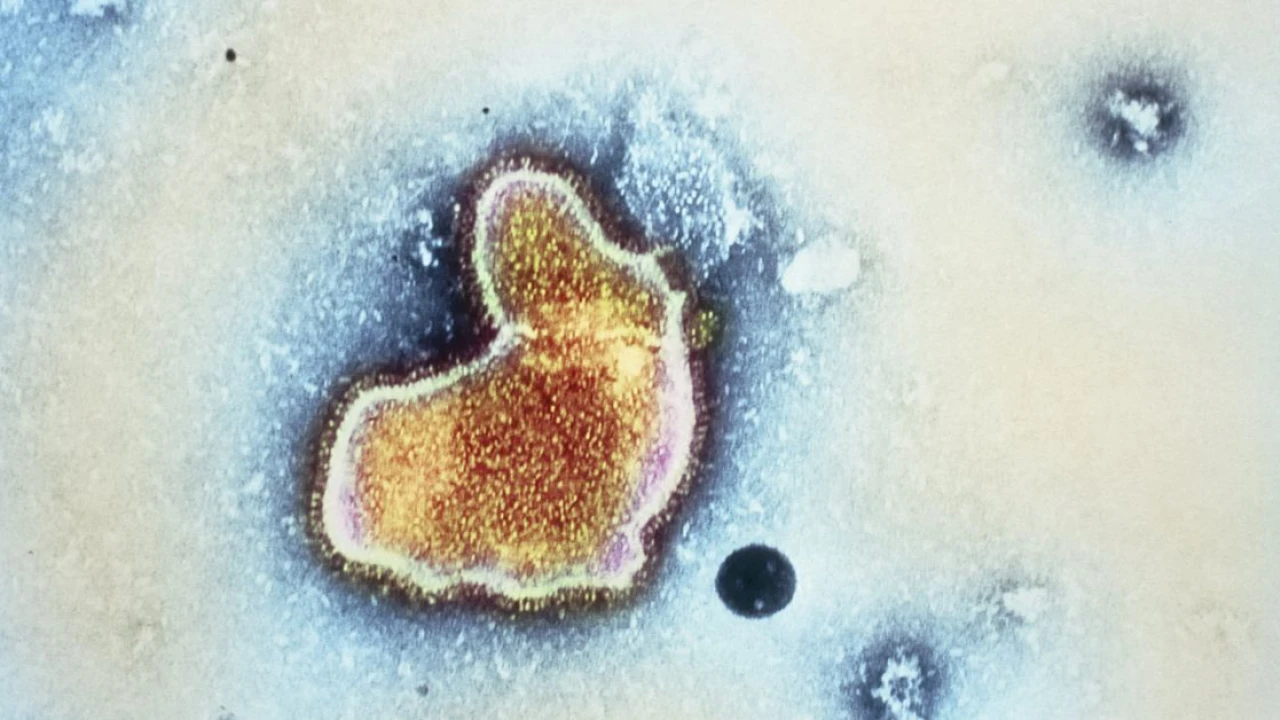
On October 13, the drug manufacturer Sanofi made a surprising announcement: Public demand for Beyfortus — the brand name of nirsevimab, the company’s new product aimed at protecting newborns from severe respiratory syncytial virus (RSV) infections — had wildly outpaced supply.
In some ways, that’s good news: This is the first RSV season that the drug has been available, and uptake has been high. Understandably so: RSV is the top cause of infant hospitalizations worldwide. Pediatricians have enthusiastically welcomed this fall’s avalanche of new vaccines and other products to help prevent the infection’s worst outcomes. And despite the fleeting rise in childhood vaccine hesitancy that took place during the pandemic, parents still trust and listen to pediatricians about vaccines.
But it also means some children have been unable to receive the immunization, and it reveals deeper, more structural problems with how the US administers childhood vaccinations.
In response to the shortage, the Centers for Disease Control and Prevention recommended on Monday that the drug be prioritized for the youngest and highest-risk babies due to the shortage. But Sean O’Leary, a pediatric infectious disease specialist at the University of Colorado’s medical school, says the shortage should never have occurred.
O’Leary serves as the American Academy of Pediatrics liaison to the CDC’s Advisory Committee on Immunization Practices. “We were consistently told that there would not be a supply problem — that there would be plenty,” he said. “And so that piece was extraordinarily frustrating for me.”
There were several other barriers O’Leary knew might impede the Beyfortus rollout, though. Inadequate supply should be a temporary speed bump in the drug’s distribution, but a different and more entrenched obstacle will likely create challenges for Beyfortus access for a while, he said: “The ridiculous way that we pay for vaccines in this country.”
How Beyfortus works
RSV is deadly to babies on a global scale. In the US alone, it causes 58,000 hospitalizations and 100 to 300 deaths each year. So when scientists finally figured out how to produce a vaccine that would protect people from the virus’s worst outcomes a few years ago, it was considered a massive breakthrough in child health.
Babies as old as 19 months who were born prematurely or have other underlying conditions are at risk for bad RSV disease. However, the risk to babies is highest in their first six months of life, and about 40 percent of American infants who died of RSV over the past few decades were otherwise healthy.
But there’s a problem with trying to vaccinate babies who are only a few months old: Their immune systems are too immature to do much in response to vaccines. In order to protect these babies, they either need to get antibodies while they’re still in the womb — by passively receiving them from their parent — or as an injection once they’re out.
Beyfortus is the latter kind of product. It’s a monoclonal antibody that does for a baby what a vaccine would do in an older child with a more robust immune system: effectively protect them from a severe RSV infection.
The CDC also recently recommended another product, a maternal vaccine called Abrysvo, to immunize babies during pregnancy. It works by stimulating antibody production in the parent that gets transferred to baby through the placenta. To be effective, it has to be given to the pregnant parent between weeks 32 and 36 of pregnancy — which means it’s too late for babies born early this fall to be protected by this vaccine.
That makes Beyfortus the only option to protect them from severe RSV.
Stocking drugs like Beyfortus is financially risky for many pediatricians
Demand for Beyfortus currently exceeds supply. But as the need for the drug becomes more predictable, and as other monoclonal RSV antibodies in development make it onto the market, we can expect supply to better meet that demand.
It’s more complicated to fix the fragmented US health care system that creates big barriers to Beyfortus access for some kids, O’Leary said. That system is structured such that many pediatricians have to take huge financial risks to keep Beyfortus in stock. For patients who get care at those practices, access will likely be a little touch-and-go until demand also stabilizes and pediatricians can better forecast how much to stock.
Why is it so risky for some pediatricians to stock certain immunization products?
It has to do with who’s paying for the products, and how much they cost. Pediatric vaccines are paid for and distributed in the US through two main mechanisms. About half of American kids get vaccines paid for by the federal government through a program called Vaccines for Children, or VFC. The program’s goal is to ensure cost isn’t a barrier to vaccinating kids, so eligibility is restricted to kids who are Medicaid-eligible, under- or uninsured, or American Indian or Alaska Native.
The other half of American kids get vaccines paid for by private insurance companies, but only after the pediatrician administers it. What insurance companies pay for each vaccine isn’t always enough to cover its full cost, and the pediatrician often doesn’t know how much an insurance company will pay them for a vaccine until after the fact.
This setup means ordering any vaccine is somewhat of a financial risk to pediatric practices. But because most vaccines are relatively cheap, and because their familiarity to most parents makes demand relatively predictable, the risk is relatively small.
The math is totally different for Beyfortus, though: One dose costs a doctor’s office nearly $500 — and as a totally novel immunization, its popularity was hard to forecast. “For a medium-sized practice, they might have to spend $250,000 to cover their patient population,” O’Leary said. “And that is not money they have lying around.”
“It’s not that pediatricians and family docs don’t want to do the right thing,” he added — but the financial risk of just keeping Beyfortus on the shelves is a barrier.
A universal vaccination program that made vaccines available across the lifespan, free of charge, would be wonderful, O’Leary said, and it’s what other industrialized countries like Canada and the United Kingdom do. “But that’s not where we are,” he said.
Clarification, October 25, 2 pm ET: This story has been updated to more accurately reflect the amount of money a source estimated a practice might spend on Beyfortus to cover its patient population.
Correction, October 25, 7:15 pm ET: A previous version of this story suggested vaccines administered in the Vaccines for Children program are given only at federally funded clinics. These vaccines are also given at private practices.












Pakistan defeat Zimbabwe with 57 runs in 1st T20I

Gandapur rejects PM’s claims of lawlessness, ineffective CTD in KP

Murad Saeed hiding in KP CM House after Nov 24 protest, claims Tarar

5-month military training of cadets commences at PMA Kakul

8 khwarij sent to hell in operations in KP from Friday

US Black Friday spending in stores and online rose 3.4% year-over-year, data showa

Winter activity and political turmoil!

Government, opposition and public!

Present regime and dengue!

The repetition of history and the hidden sciences!

"Don't panic!"

Whispers, rumors and rulers' narrative!

چیمپیئن ٹرافی کا معاملہ۔۔!ماہراسپورٹس حافظ عمران کا بھارتی صحافی کومنہ توڑجواب!#KhabarHai #SaeedQazi

"بھارت آئے نہ آئے،چیمپیئنزٹرافی پاکستان میںہی ہوگی"اہم میٹنگ,کیاہونے جارہاہے؟عاقب قریشی اندرکی خبر

پاکستانی کھلاڑی لمبی اننگزکیوں نہیں کھیل پاتے؟سلمان بٹ کی گفتگو#GNN #GNN_Updates #SportsFlix

چیمپیئنزٹرافی نزدیک،پاکستانی کرکٹ ٹیم پرسابق کپتان سلمان بٹ کاماہرانہ تجزیہ#GNN #GNN_Updates

ہرطرف گندگی کاڈھیر،حکومت ناکارہ!"نئی نسل آوازاٹھائے گی،امپوسیبل"شہری بابا حکومت پرآگ بگولہ ہو گیا!

اسلام آباد ہائیکورٹ میں پی ٹی آئی کا احتجاج روکنے کے لیے درخواست پر سماعت #gnn #news #breaking
-

 Pakistan 1 day ago
Pakistan 1 day ago57 years of PPP, Bilawal to address Foundation Day ceremony
-

 Pakistan 2 days ago
Pakistan 2 days agoPakistan condemns Israeli atrocities in Palestine
-

 Sports 1 day ago
Sports 1 day agoCricketer dies of heart attack during live match
-

 Pakistan 2 days ago
Pakistan 2 days agoGandapur rules out row with Bushra Bibi
-

 Pakistan 1 day ago
Pakistan 1 day agoGovt hikes petrol, diesel prices for next fortnight
-

 Pakistan 1 day ago
Pakistan 1 day agoBilawal Bhutto says Govt has not consulted PPP over ban on any party
-

 Pakistan 1 day ago
Pakistan 1 day agoOperational issues: Four PIA flights canceled, 36 delayed
-

 Business 1 day ago
Business 1 day agoLPG becomes more expensive